
Supporting Your Patients Between Visits
At TaskferHealth, we ensure that your patients receive continuous support and care, even when they’re not in the office.
Chronic Care Management
CCM is a Medicare reimbursement program that allows Taskfer Health to receive monthly payments for the ongoing non-face-to-face care coordination already provided to patients with multiple chronic conditions
- Billable monthly — no devices, no hardware costs
- Covers care plans, medication management, and provider coordination
- Stackable with RPM and BHI for combined $300–400/patient/month
By CCN Health Clinical Team · Last Updated April 2026
What is CCM?
Chronic Care Management (CCM) is a comprehensive approach to managing patients with multiple chronic conditions. It involves coordinated care and regular check-ins to improve health outcomes and enhance patient engagement.

Who Qualifies for CCM?
How CCM Fits Into Your Practice

how it works
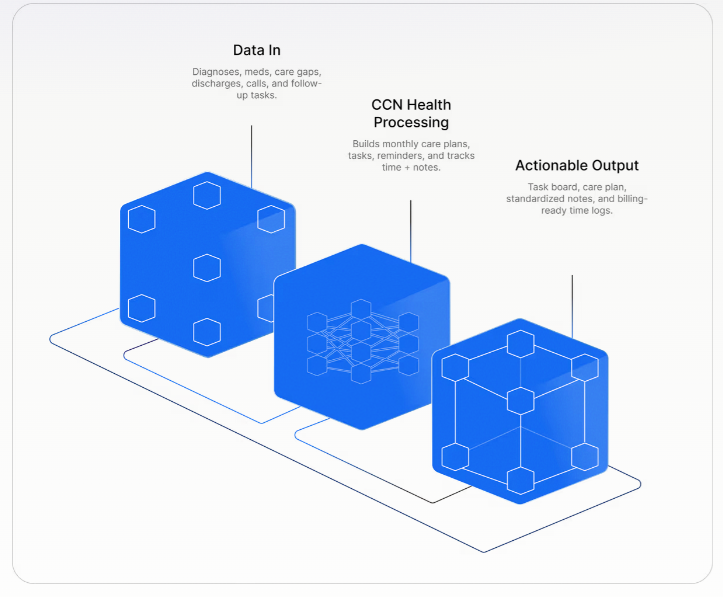
How Our CCM Program Works
Patient Identification & Enrollment
We assist in identifying patients who qualify for CCM and handle the enrollment process, ensuring a smooth transition into the program.
Care Plan Development
Working closely with your healthcare team, we develop personalized care plans tailored to each patient’s needs, promoting better health management.
Monthly Care Coordination
Our U.S.-based chronic care managers coordinate monthly check-ins, providing essential support and ensuring adherence to care plans. We act as an extension of your staff, maintaining communication with patients.
Continuous Monitoring & Reporting
We continuously monitor patient progress and report findings back to your team, ensuring that care remains consistent and effective. Our goal is to keep your patients engaged and informed throughout their care journey.
how it works
Patient Criteria
Two or more chronic conditions
Each must be expected to last at least 12 months (or until death) and place the patient at significant risk of death, acute exacerbation, or functional decline.
Medicare Part B enrollment
The patient must be enrolled in traditional Medicare Part B. Many Medicare Advantage plans also reimburse CCM, though coverage varies by plan.
Patient consent
Verbal or written consent must be obtained and documented before CCM services begin. The patient must be informed about cost-sharing (standard 20% coinsurance) and the single-provider billing rule.
Initiating visit within 12 months
An in-person E/M visit, Annual Wellness Visit (AWV), or Initial Preventive Physical Exam (IPPE) must have occurred within the prior year.
Comprehensive care plan
An electronic, person-centered care plan must be established covering all chronic conditions, medications, treatment goals, and coordination needs.
One provider per month
Only one practitioner or practice may bill CCM for a given patient in any calendar month.
Overview
What is Chronic Care Management
Chronic Care Management (CCM) is a Medicare reimbursement program that pays providers for the non-face-to-face care coordination they deliver to patients who have two or more chronic conditions. These are phone calls, care plan updates, medication reviews, and provider check-ins that happen between office visits — work that historically went unbilled.
CMS created the CCM program in 2015 because chronic conditions account for over 93% of Medicare spending, and patients with multiple conditions often fall through the cracks between specialists. CCM gives practices a financial model to assign dedicated staff to coordinate care proactively — reducing hospitalizations, ER visits, and medication errors.
Unlike Remote Patient Monitoring (RPM), CCM does not require any devices. It is purely a care coordination service: developing care plans, reconciling medications, communicating with other providers, and educating patients. Clinical staff perform these activities under general supervision, meaning the physician does not need to be on-site — making CCM one of the most scalable Medicare programs available.
📊 KEY FACTS AT A GLANCE
Non-face-to-face care coordination
2+ chronic conditions, 12+ months
20 minutes/month (clinical staff)
None — no hardware needed
99490, 99439, 99491, 99437, 99487, 99489
$66–$222 per patient/month
General (nurse/MA can perform)
RPM + BHI ($300–400/mo combined)
Verbal or written, one-time
Programs
Run all programs on one platform
Remote Patient Monitoring.
Real-time vital sign monitoring with FDA-cleared devices
RPM Billing Codes
-
99453
~$19
Setup & Education
One-time per patient enrollment
-
99454
~$55/mo
Device Supply (16+ days)
16+ readings in 30-day period
-
99445
~$55/mo
Device Supply (2–15 days)
2–15 readings in 30-day period new 2026
-
99457
~$50/mo
Clinical Review (20+ min)
First 20 min of clinical staff time
-
99470
~$25/mo
Clinical Review (10 min)
First 10 min of clinical staff time new 2026
-
99458
~$42/mo
Additional Review
Each additional 20 min (add-on to 99457)
Chronic Care Management.
Care coordination for patients with chronic conditions
CCM Billing Codes
-
99490
~$62/mo
CCM Services
20+ min of clinical staff time
-
99491
~$86/mo
Complex CCM
60+ min of physician/QHP time
-
99439
~$47/mo
Additional 20 min
Each additional 20 min of staff time
Remote Therapeutic Monitoring.
Monitoring for musculoskeletal and respiratory therapy
RTM Billing Codes
-
98975
~$19
Setup & Education
One-time initial device setup
-
98976
~$50/mo
Respiratory RTM
16+ days respiratory data
-
98977
~$50/mo
MSK RTM
16+ days MSK therapy data
-
98980
~$48/mo
Treatment Mgmt
First 20 min treatment management
-
98981
~$38/mo
Additional Mgmt
Each additional 20 min
Qualifying Chronic Conditions
Any two conditions from the categories below can qualify a patient for CCM, as long as each is expected to last 12+ months and places the patient at significant risk.
Cardiovascular
- Hypertension I10
- Congestive Heart Failure I50.x
- Coronary Artery Disease I25.x
- Atrial Fibrillation I48.x
- Peripheral Vascular Disease I73.9
Endocrine & Metabolic
- Type 2 Diabetes E11.x
- Type 1 Diabetes E10.x
- Obesity E66.x
- Hypothyroidism E03.9
- Hyperlipidemia E78.x
Respiratory
- COPD J44.x
- Chronic Asthma J45.x
Renal
- Chronic Kidney Disease (Stages 1–5) N18.x
Neurological & Cognitive
- Alzheimer's Disease / Dementia G30.x / F03.x
- Parkinson's Disease G20
Behavioral Health
- Major Depressive Disorder F33.x
- Generalized Anxiety F41.1
- Substance Use Disorders F10–F19
Musculoskeletal
- Osteoarthritis M15–M19
- Rheumatoid Arthritis M05–M06
- Osteoporosis M80–M81